WPW syndrome:副傳導路徑 (Accessory pathway)如何定位?
WPW syndrome具有先天的副傳導路徑,有心因性猝死風險,盛行率為0.1-3.0 (每千人)。
副傳導路徑可以順向 (anterograde)或逆向 (retrograde),兩個方向都允許,單純逆向或順向都比較少見 (單純逆向佔15%)。
當折返迴路 (re-entrant circuit)發生在副傳導路徑時,就會引發頻脈心率不整 (AVRT)。
註1:WPW = Wolff-Parkinson-White; AVRT = atrioventricular reentry tachycardias
作者:張庭嘉
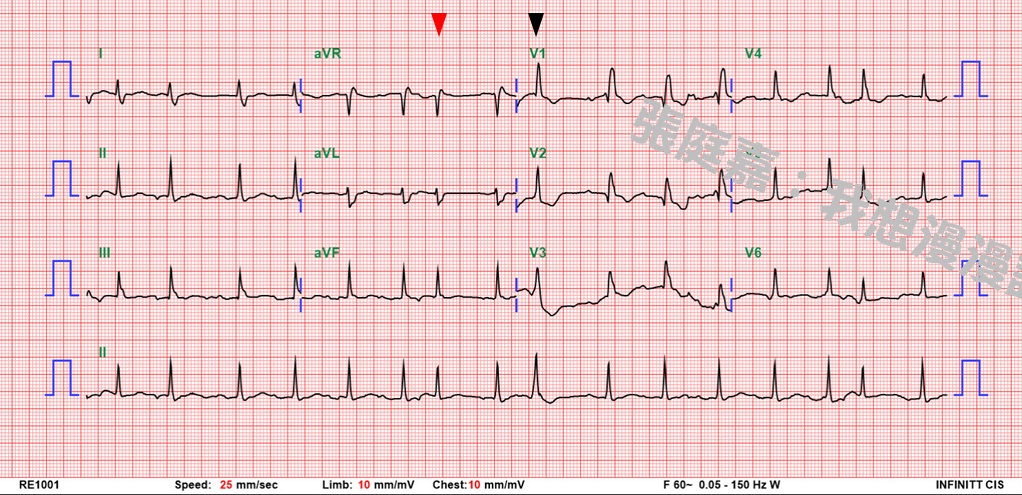
WPW的EKG特徵包括PR interval短 (< 120 ms)、delta wave、QRS寬 (> 110 ms);
另外ST segment和T波會有反向 (discorfant)的特徵,也可見在前胸或下壁導程中假的Q wave (實際上是負向的delta波)。
註2:Discordant表示與QRS complex主要的方向相反
不過副傳導路徑到底在哪裡,應該怎樣去定位呢?(以下是107年醫師二階國考的題目)

一般可簡單把WPW分為Type A及Type B,前者在胸前導程會有正向的delta波,並且V1的R/S會大於1;
後者則在V1和V2有負向的delta波。
Type A代表左側的副傳導路徑;Type B代表右側的副傳導路徑。
副傳導路徑理論上可以位於AV ring (groove)或septum的任意位置;
最常見的副傳導路徑位於left lateral (50%),其次是posteroseptal (30%)、right anteroseptal (10%)、right lateral (10%)。
不過僅僅知道這些要答題還遠遠不夠...
許多研究探討副傳導路徑的所在,有各樣的flow chart,不過同樣傳導路徑也不會每次都產生同樣的pattern,甚至有少數 (13%)的個案並不是只擁有一條副傳導路徑。

這題在V1的R/S小於0.5,R/S在V2又大於0.5,故副傳導路徑的位置應在RPL/RP處。(近PS)
Goldberger's上簡單把副傳導路徑在lateral part of LV者,它的delta波在左側導程 (I, aVL, sometimes V6)是負向的,在右側導程則是正向 (V1, V2)
位於心室後壁 (posterior)者,則胸前導程會是正向的delta波,下肢導程則會是負向的。(很像判斷下壁梗塞那樣)
右側free wall者,QRS在V1、V2是明顯負向的 (自右側傳來),配上biphasic或有點負向的delta波,然後QRS在V6是正向的。
Anteroseptal副傳導路徑是最罕見的類型,於V1、V2會有負向的delta波。
2. Goldberger's Clinical Electrocardiography: A Simplified Approach, 9/e > Atrioventricular (AV) Conduction Disorders, Part II: Preexcitation (Wolff–Parkinson–White) Patterns and Syndromes
3. Taguchi N, Yoshida N, Inden Y, et al. A simple algorithm for localizing accessory pathways in patients with Wolff-Parkinson-White syndrome using only the R/S ratio. J Arrhythmia . 2014;30:439–443.
副傳導路徑可以順向 (anterograde)或逆向 (retrograde),兩個方向都允許,單純逆向或順向都比較少見 (單純逆向佔15%)。
當折返迴路 (re-entrant circuit)發生在副傳導路徑時,就會引發頻脈心率不整 (AVRT)。
註1:WPW = Wolff-Parkinson-White; AVRT = atrioventricular reentry tachycardias
作者:張庭嘉
WPW的EKG特徵包括PR interval短 (< 120 ms)、delta wave、QRS寬 (> 110 ms);
另外ST segment和T波會有反向 (discorfant)的特徵,也可見在前胸或下壁導程中假的Q wave (實際上是負向的delta波)。
註2:Discordant表示與QRS complex主要的方向相反
不過副傳導路徑到底在哪裡,應該怎樣去定位呢?(以下是107年醫師二階國考的題目)
一般可簡單把WPW分為Type A及Type B,前者在胸前導程會有正向的delta波,並且V1的R/S會大於1;
後者則在V1和V2有負向的delta波。
Type A代表左側的副傳導路徑;Type B代表右側的副傳導路徑。
副傳導路徑理論上可以位於AV ring (groove)或septum的任意位置;
最常見的副傳導路徑位於left lateral (50%),其次是posteroseptal (30%)、right anteroseptal (10%)、right lateral (10%)。
不過僅僅知道這些要答題還遠遠不夠...
許多研究探討副傳導路徑的所在,有各樣的flow chart,不過同樣傳導路徑也不會每次都產生同樣的pattern,甚至有少數 (13%)的個案並不是只擁有一條副傳導路徑。
用EKG來定位副傳導路徑
Braunwald's有節錄自Taguchi N研究的判別流程圖(如下圖):
這題在V1的R/S小於0.5,R/S在V2又大於0.5,故副傳導路徑的位置應在RPL/RP處。(近PS)
Goldberger's上簡單把副傳導路徑在lateral part of LV者,它的delta波在左側導程 (I, aVL, sometimes V6)是負向的,在右側導程則是正向 (V1, V2)
位於心室後壁 (posterior)者,則胸前導程會是正向的delta波,下肢導程則會是負向的。(很像判斷下壁梗塞那樣)
右側free wall者,QRS在V1、V2是明顯負向的 (自右側傳來),配上biphasic或有點負向的delta波,然後QRS在V6是正向的。
Anteroseptal副傳導路徑是最罕見的類型,於V1、V2會有負向的delta波。
參考資料
1. Clinical Arrhythmology and Electrophysiology: A Companion to Braunwald's Heart Disease, 3/e > Typical Atrioventricular Bypass Tracts2. Goldberger's Clinical Electrocardiography: A Simplified Approach, 9/e > Atrioventricular (AV) Conduction Disorders, Part II: Preexcitation (Wolff–Parkinson–White) Patterns and Syndromes
3. Taguchi N, Yoshida N, Inden Y, et al. A simple algorithm for localizing accessory pathways in patients with Wolff-Parkinson-White syndrome using only the R/S ratio. J Arrhythmia . 2014;30:439–443.